CEREBRAL PALSY :
Cerebral palsy is considered a neurological disorder caused by a
non-progressive brain injury or malformation that occurs while the
child’s brain is under development. Cerebral palsy primarily affects
body movement and muscle coordination. Though cerebral palsy can be
defined, having cerebral palsy does not define the person that has the
condition.It is a term used to describe broad spectrum of motor disability which is non-progressive and is caused by damage to the brain at or around the birth.
It is a disorder which develops due to damage to central nervous system and this damage can take place before,during or after birth of the child.
- Cerebral palsy is not a disease, it is actually a term used to describe a range of conditions that typically cause physical impairment.
- CAUSES:
- Antenatal causes:
- Genetic causes:
- intrauterine virus infection like rubella cytomegalovirus infections:
- hypoglycemia:low blood sugar
- trauma and infections to the mother:
- Neonatal causes:
- prematurity:
- vascular causes: occlusion of the internal carotid or midcerebral artery during birth
- trauma:
- asphyxia:
- Postnatal causes:
- delayed cry:
- severe jaundice:
- TOPOGRAFICAL CLASSIFICATION:
- Monoplegia: one limb affected.
- Diplegia: Involvement of four limbs with leg more affected.
- Triplegia: Involvement of three limbs.
- Quadriplegia: Involvement of four limbs with arms more affected.
- Hemiplegia:one side of the body paralysed
- Paraplegia: Involvement of both the legs only.
- ACCORDING TO TYPES:
- Spastic: spasticity seen in cerebral palsy is usually clasp knife.
- Ataxic:
- Athetoid:
- Mixed :
development is a progression through which one attains maturity and is a continuous and orderly process.
When child is born tracts are unmyelinated hence isolation and inhibition are not possible. As myelination occurs child can carry out isolated movements. hence neonates develops from generalized to specific behaviour. It is at this stage that various primitive reflex patterns also become apparent.
PRIMITIVE REFLEX PATTERNS:
This refxes are classified according to the level at which they are controled.
- spinal cord
- brainstem
- midbrain
- cortex
- automatic reflex
- SPINAL REFLEX
flexor withdrawl
2. Extensor thurst:
position: supine head neutral one leg flexed nd other is extended
stimulus: sole of flexed leg
responce: immidiate extension adduction and internal rotation of flexed leg.
3.Cross extensor:
position:supine head neutral one leg extended and other is flexed.
stimulus: medial aspect of extended leg.
responce: immidiate extensio adduction and internal rotation of flexed leg with plantar flexion of foot.
present since birth and integrate on 2 months.
4. Palmar grasp:
stimulus: press some object on palm from ulnar side.

responce: grasping of the object on the ulnar side.
5. Plantar grasp:
stimilus: press some object on the plantar side of toes lateraly:
responce: clawing and clutching.

palmar and plantar both reflexes are present since birth and integrate on 10 months.
6.sucking and rooting:
stimulus: finger touching or going into child's mouth.
responce: turning of head of the child in the direction of stimulus.
present at birth and integrates within 3 to 6 months.

BRAINSTEM LEVEL:
ASYMMETRICAL TONIC NECK REFLEXS:
position: supine head neutral and limbs relexed.
stimulus: turning of head of child towards one side.
responce: extension of limbs on face side and flexion of the limb on occipital side.
present at 2 months of age and integrated by 4 to 6 months.

2. SYMMETRICAL TONIC NECK REFLEX
position: quadripedal position.
stimulus: head is either flexed or extended.
responce: when head is in flexion, the UPPER LIMB gets FLEXED and LOWER LIMB EXTENDS, similarly when the head is extened the UPPER LIMBS goes in to a FLEXED.
this reflex is present from 4 months and disappear by 6 months.
3. TONIC LABYRINTHINE REFLEX:
 position: either supine or prone:
position: either supine or prone: stimulus: position itself is stimulus.
prone reflex responce: when child is in supine position then there is increase in tone in the extensor group of muscles and when child kept in prone position then there is increase tone of flexor group of muscles.
present from birth to 3 to 4 months.
4. POSITIVE SUPPORTING REACTION:
stimulus: hold child in erect position, lift him up and bounce up down on plinth till sole of foot touches the plinth.
responce: exaggerated extension of the foot touches the plinth.
present at birth and integrated by 4 months.

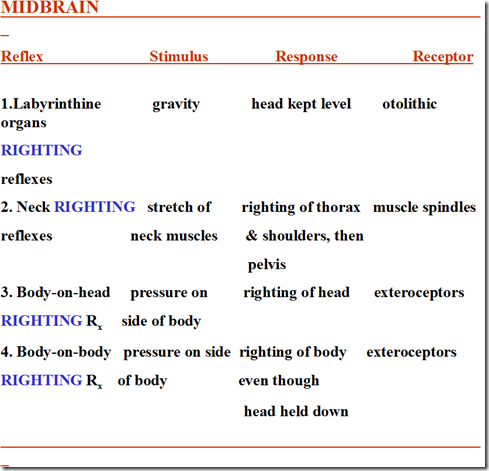
MIDBRAIN LEVEL REFLEXES:

- TREATMENT:Physical therapy is a branch of rehabilitative health that is
considered one of the most important aspects of treating children with
cerebral palsy. Those with cerebral palsy experience mobility,
function, posture and balance challenges of varying degrees, and
physical therapy – which focuses on basic mobility such as standing,
walking, climbing stairs, reaching or operating a wheelchair – is a key
element in the multidisciplinary approach to increasing a child’s
mobility.
Physical therapy is the rehabilitation of physical impairments by training and strengthening a patient’s large muscles – those in the arms, legs, and abdomen. The goal of physical therapy is to maximize functional control of the body, or increase gross motor function.
The goal of physical therapy is to help individuals: - develop coordination
- build strength
- improve balance
- maintain flexibility
- optimize physical functioning levels
- maximize independenceAt the start of physical therapy, a comprehensive medical history for
the child will be obtained. Additionally, the therapist will conduct a
series of tests, observations and measurements to assess the child’s
body mechanics and function.
The examination may assess: - Gait
- Range of joint motion
- Physical strength
- Flexibility
- Balance
- Endurance
- Joint integrity
- Posture
- Neuromoter development
- Sensory integration
- Cognitive functioning
- Reflexes
- Breathing, respiration
No comments:
Post a Comment